
Growth modulation in Genu Valgum secondary to Multiple Hereditary Exostosis
Article Sidebar
Main Article Content
Abstract
Objective: Hereditary Multiple Exostoses (HME) is a rare disease with a prevalence of 1:50,000, which can manifest in various ways. This cartilaginous tumor can appear in a spectrum, ranging from mobility restriction to chronic pain and alignment disorders. Literature often describes forearm deformities such as excessive radial bowing, ulnar shortening, and radial head dislocation. Factors resulting in genu valgus and specific treatment strategies are not frequently studied. Considerations specific to the disease, such as the morphology of the lesion, time taken for deformity correction, and timing of exostosis excision, should be taken into account when treating genu valgum in patients with MHE.
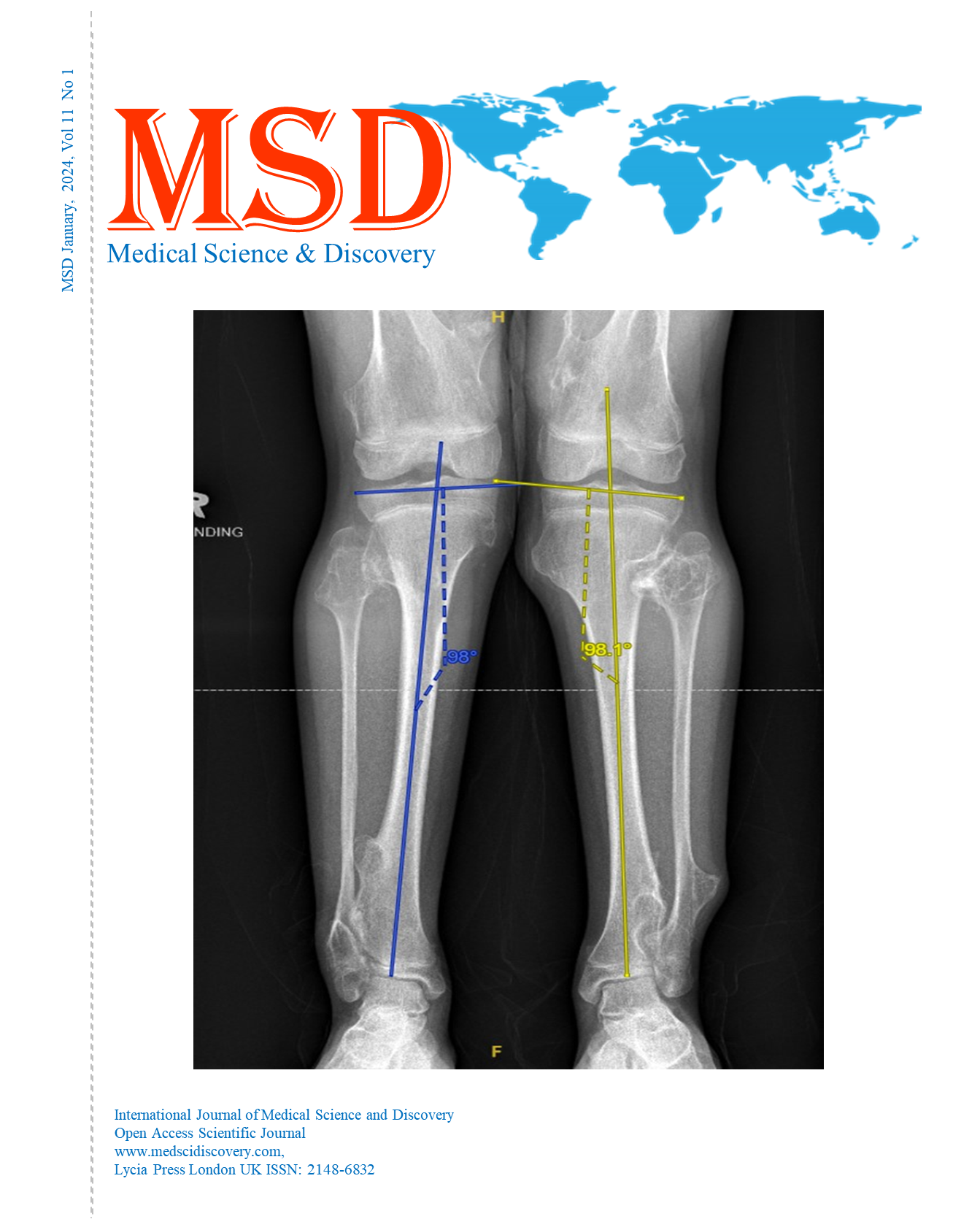
Case: Our case report highlights a teenager with underlying MHE who presented to us with "knock knees" since childhood. Clinically, it was observed that the patient had bilateral genu valgum and multiple bony swellings overlying the proximal tibia and distal femur. The deformity was subsequently addressed with bilateral proximal tibia hemi-epiphysiodesis, exostoses excision of bilateral proximal tibia, and left distal tibia. The radiographs and surgical technique are detailed in the case report. Our literature review indicates that distal femur exostoses play a significant role in causing genu valgus in these patients. The morphology of the exostoses also affects the development of genu valgus, with sessile lesions contributing more bony deformity compared to pedunculated lesions. Hemi-epiphysiodesis, as performed in our patient, often achieves outcomes similar to idiopathic genu valgum. However, the correction would take about 6 months longer, so in cases of MHE, correction should start earlier. Another dilemma in cases of pathological genu valgus is whether to remove exostosis during corrective surgery. Literature advocates delaying the excision of proximal tibia exostoses as long as possible to reduce the risk of accelerating deformity worsening.
Conclusion: In conclusion, factors influencing genu valgus progression include the morphology of the lesion (sessile), presence of metaphyseal flaring, and a history of prior exostosis excision. Early detection of the pathology would yield better outcomes, as the rate of deformity correction in children with MHE is slower due to abnormal physis. Meticulous surgical technique to prevent injury to the physis and knee immobilization post-excision of exostosis are important factors in preventing the development of genu valgus in children with MHE.
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Accepted 2024-01-19
Published 2024-01-30
References
Lower Limb Deformities and Limb Length Discrepancies in Hereditary Multiple Exostoses. Madoki et al, 2022. Acta Orthopedica Belgica
Hereditary Multiple Exostoses: Current Insights. Arrienzo et al.Dove press Journal: Orthopaedic research and reviews .February 2023
The Development of tibiofemoral Angle in Children. Salenius et al. 1975. Journal of Bone, Joint and Surgery
Potential Influence of factors for Genu valgus with hereditary multiple Exostoses. Liu et al. July 2022 Journal of Peadiatric Orthopaedics.
Rapidly Acquired Valgus Deformity of the knee after osteochondroma resection in Multiple hereditary exostoses patients. A report of two cases. Alexandra et al. November 2021