
Development of Cerebral Infarction After Stripping of Vena Saphena Magna: Case Report
Article Sidebar
Main Article Content
Abstract
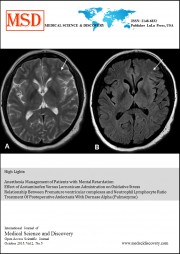
Cerebrovascular disease is the most frequent cause of neurological diseases. Embolic infarction is one of the most common causes of stroke. In the majority of patients with cerebral embolism, it is shown that emboli mostly originate from the heart via arterial circulation. Embolism rarely occurs as a paradoxical embolism through atrial / ventricular septal defect (ASD/VSD) or patent foramen ovale (PFO). In our clinical case, cerebral infarction is caused by ASD after vena saphena magna (VSM) stripping. Thirty- four- year- old female patient was admitted with motor and sensory loss at left lower extremity below the knee after stripping of VSM. Detailed neurological examination was done. She had left foot motor deficit, anesthesia of left lower extremity below the knee, impairment of motor strength (0/5 dorsiflexion and plantar flexion) of the left foot. After radiological investigation, diffusion-weighted magnetic resonance imaging (MRI) revealed several, millimetric, nonspecific, nodular signal changes in some parts of bilateral periventricular, subcortical white matter of the brain that showing no diffusion limitation. In systematic examination, atrial septal defect was detected by echocardiography. Patient was treated with anticoagulant therapy. This case highlights detailed cardiological examination should be done in patients with cerebral infarction
Downloads
Article Details
References
Ropper A. H, Brown R. H. Adams and Victor’s Principles of Neurology. In: Togay Işıkay C., editor. 8th ed. Vision Disorders.2006: 209.
Abu Rahma AF, Richmond BK., Robinson PA. Etiology of peripheral arterial tromboembolism in young patients. American Journal of Surg. 1998; 176: 158-161.
Seğmen H, Kayım Ö., Bolayır E. Echocardiographic findings in young ischemic patients.Journal ofCumhuriyet University Faculty of Medicine2007; 29 : 109-112.
Crump R, Shanding AH., Van nata B. Ellestad M. Prevalance of patient foramen ovale in patients with acute myocardial infarction and angiographically normal coronary arteries. American Journal of Cardiol. 2000; 85 : 1368-70.
Ash N, Lubetsky A, Ezra D, Olchovsky D. Atrial septal defects and embolic stroke inyoung adults. Harefuah. 1992 Aug;123(3-4):91-4, 155.
G. Devuyst, J. Bogousslavsky. Status of Patent Foramen ovale, Atrial Septal Aneurysm, Atrial Septal Defect and Aortic Arch Atheroma as Risk Factors for Stroke.Neuroepidemiology 1997;16: 217-223.
Refah Sayın, Tezay Çakın Güleç, Temel Tombul A Case with Atrial Septal Defect, retinal artery occlusion and Cerebral Infarction.Van Medical Journal: 16 (3):109-112, 2009.